

- 874.50 KB
- 2022-05-26 16:47:14 发布
- 1、本文档共5页,可阅读全部内容。
- 2、本文档内容版权归属内容提供方,所产生的收益全部归内容提供方所有。如果您对本文有版权争议,可选择认领,认领后既往收益都归您。
- 3、本文档由用户上传,本站不保证质量和数量令人满意,可能有诸多瑕疵,付费之前,请仔细先通过免费阅读内容等途径辨别内容交易风险。如存在严重挂羊头卖狗肉之情形,可联系本站下载客服投诉处理。
- 文档侵权举报电话:19940600175。
TherapeuticsinRenalDiseaseDrMichaelClarksonConsultantRenalPhysician–CUH
ChronicKidneyDiseaseCommonEasytoDiagnoseEffectiveTherapiesAvailableCKDCareSuboptimal
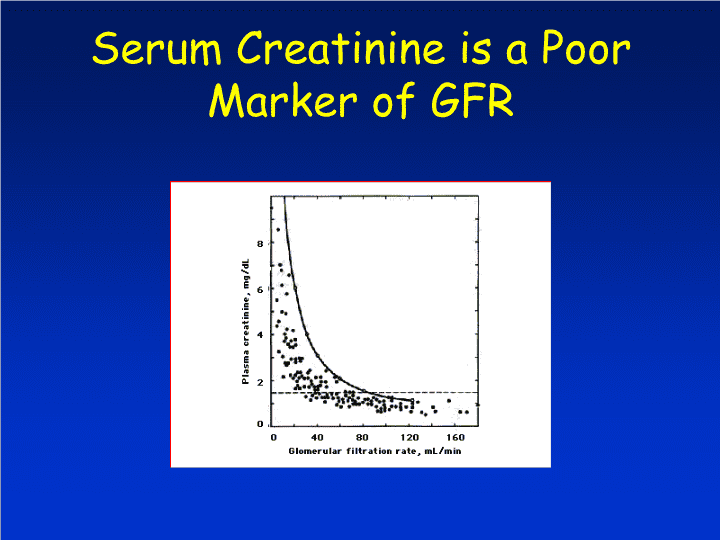
SerumCreatinineisaPoorMarkerofGFR
MDRDeGFRMDRDequation–ComplexlogrhythmicequationIntegrateskeyvariablesAgeSexCreatinineRaceUreaAlbumin
GFRistheacceptedmeasureofkidneyfunctionGFRisdifficulttoinferfromserumcreatininealoneAutomaticreportingidentifiesCKDpatientswithapparently“normal”serumcreatinineReducesbarriertoearlydetectionMDRDeGFR
ThreesimpletestsidentifyCKDinadultsDipstickUrinalysis–Haematuria/MacroalbuminuriaUrinePCR-Urineproteintocreatinineratioona“spot”urinesample24-hoururinecollectionsareNOTneededeGFR-EstimatedGFRfromserumcreatinineusingtheMDRDequation
SpotRatios!24hourcollectionscumbersomeExcretionofcreatinineandproteinisreasonablyconstantthroughoutthedayArandomurineprotein:creatinineratiohasbeenshowntocorrelatewitha24-hrestimationExpressedeitherasmg/mg(easy)ormg/mmol(multiplyx0.0088)
SpotRatios!24yoladywithankleoedema,proteinuriaandhypercholesterolaemiaSpoturineprotein924mg/LSpoturinecreatinine3343µmol/LRatio=276mg/mmol(normal:0-45)Converttomg/mg(276x0.0088)=2.4g/24hr
IdentifyingCKDBISHBASHBOSH
StagingofChronicKidneyDisease
StageDescriptionGFREvaluation/Plan0Atrisk>90Modifyriskfactors1Kidneydamage/>90Diagnose/Treatcause.SlownormalGFRprogressionandevaluateCVrisk.2Mild60-89Estimateprogression3Moderate30-59Evaluateandtreatcomplications4Severe15-29PrepareforRRT5ESRD<15InitiateRRTNKF,USA
FactorsMediatingEvolutionofCKDSusceptibilityFactorsInitiationFactorsProgressionFactors
SusceptibilityFactorsMalegenderHypertensionAge1ml/yearlossnormallyGeneticBackgroundACEpolymorphismsReducedNephronMassatBirth
DiabeticNephropathy>GlomerularDisease>TubulointerstitialDisease>HypertensiveNephrosclerosisInitiationFactors
ProgressionFactorsProgressivelossofrenalfunctionwilloccurevenintheabsenceofovertactivityoftheprimaryrenaldisorder
ProgressionFactorsHypertensionGlomerularHypertensionProteinuriaHyperlipidemiaGeneticFactorsMiscellaneousExacerbatingEffectofRiskFactorClustering
MaladaptiveResponsetoLossofNephronMassInitialRenalInsultLossofNephronMassCompensatoryGlomerularHypertrophy/HyperfiltrationMaximisationofGFRIntraglomerularHypertensionPodocyteInjury/MesangialMatrixExpansionSecondaryFSGSProteinuria/HypertensionRAASBlockadeBPControlDietaryProteinRestriction
HypertensionandCKD
RoleofHypertensioninCKDProgression50-75%ofpatientswithCKDhaveBP>140/90mmHgGoalsoftherapyRetardCKDprogressionReduceoverallcardiovascularrisk
RoleofHypertensioninCKDProgressionStrongassociationwithpoorrenaloutcomesesp.indiabeticnephropathyMicroalbuminuriaprogressionMorphologicinjuryPredictslossofrenalfunctioninnon-diabeticglomerulardisordersandinAPKD.Confoundingeffectofproteinuriamakeaccurateassessmentofindependenteffectdifficult
HypertensionandCKDTargetBloodPressure
RelationshipbetweenBPControlandRateofDeclineinGFRBakrisetalAJKD,2000.
DeclineinGFRandHTN:StratificationforProteinuriaMDRDStudy:ArchIntMed,1995
EffectiveControlofHypertensioninCKD:
MultipleAgentsRequiredBakrisetalAJKD,2000
EffectiveControlofHypertensionYieldsMajorBenefitinCKD
Earlytreatmentcanmakeadifference100100NoTreatmentDelayedTreatmentEarlyTreatment47914KidneyFailureGFR(mL/min/1.732)283
BloodPressureGoalsinCKDStratifyAccordingtoProteinuriaProteinuria<3gGoal<130/80Proteinuria>3gGoal<125/75OptimalBloodPressureUnknownDiureticsEssential120/80??
ProteinuriaandCKD
MicroalbuminuriaandMacroalbuminuriaMicroalbuminuriaMacroalbuminuriaDefinition>30-299mg/day>300mg/dayRoutineDipstickNegativePositiveRenalSignificanceRiskMarkerMarkerofprogressionCardiovascularRiskIncreasedIncreased
MaladaptiveResponsetoLossofNephronMassInitialRenalInsultLossofNephronMassCompensatoryGlomerularHypertrophy/HyperfiltrationMaximisationofGFRIntraglomerularHypertensionPodocyteInjury/MesangialMatrixExpansionSecondaryFSGSProteinuria/Hypertension
ProteinuriaandCKDProteinuriaevaluationmandatoryinallpatientswithCKDIndependentriskfactorforCKDprogressionBestpredictorofESRD
AdverseConsequencesofProteinuriavsloweGFRAll-CauseMortality(per1000patientyrs–rate(95%CI))NormalMildHeavyeGFR>602.7(2.6-2.8)5.8(5.5-6.0)7.2(6.6-7.8)eGFR45-592.9(2.7-3.0)5.2(5.5-6.0)7.2(6.5-7.8)eGFR30-444.0(3.7-4.2)5.8(5.4-6.2)7.5(6.8-8.2)eGFR15-306.7(6.2-7.3)9.1(8.2-10.0)10.4(9.3-11.6)Hemmelgarnetal.JAMA.2010;303(5):423-429.
ProteinuriaInCKDInterventionStudiesPharmacologicApproachesDietaryApproaches
ReductioninproteinuriaReductioninproteinuriaiskeytosuccessfulrenoprotectivestrategy.Anti-hypertensiveregimenswithbetterreductioninproteinuriaaffordgreaterrenoprotectivebenefits.BenefitpersistsevenwhenBPwithinthe‘normalrange’.
ProteinuriaandCKDPharmacologicApproaches
ACE-IDecreaseProteinuriaMorethanConventionalAnti-HypertensiveTherapyJafaretal,MetaAnalysisAnnIntMed2001
RAASBlockadeinCKD-
MechanismofActionReductioninintraglomerularhypertensionEfferentarteriolarvasodilatationImprovedglomerularpermselectivityAttenuationofAII-stimulatedgrowthfactorandinflammatorycytokinesecretionPreventionofextracellularmatrixaccumulation
AfferentEfferentVasodilatorsProstaglandinsNitricOxideVasoconstrictorsEndothelinCatecholaminesAdenosineVasoconstrictorsAngiotensin-II
AfferentEfferentVasodilatorsProstaglandinsNitricOxideVasoconstrictorsAngiotensin-IIPGcHyperfiltrationMechanicalStrain2ºFSGS
EfferentRAASBlockadePGcHypertensionControlBPLowerGFRReductioninProteinuria
AngiotensinRecptorBlockade
MoreRisk,MoreBenefit!
InitiationofACE-IorARB“AlthoughACEinhibitorsnowhaveaspecialisedroleinsomeformsofrenaldiseasetheyalsooccasionallycauseimpairmentofrenalfunctionwhichmayprogressandbecomesevereinothercircumstances”BNF
InitiationofACE-IorARBCaseExample42yearoldladyHypertensionRecurrentUTIAtrophicleftkidneyPre-eclampsiax2BP=155/95MAP=115SeCr=145umol/L.MDRDGFR=50ml/minUrineProteintoCreatinineratio:1.4
InitiationofACE-IorARBInitiatedonRamipril5mgqd+lowsaltdietDay7.BP=145/90Ramiprilincreasedto10mgqdDay14BP140/85RepeatCreatinine=175umol/L,K+5.4mmol/LEstimatedGFR=42mls/min
InitiationofACE-IorARBClinicalDilemmaSubstantialfallinGFRfollowingRAASblockadeHyperkalaemiaDonotsuspectrenovasculardiseaseWithdrawACE-I/ARB?
InitiationofRAASBlockade:
InitialreductioninGFRpredictsbetteroutcomeAperlooetal,KidInt,1997
InitiationofACEi/ARB10010047914KidneyFailureGFR(mL/min/1.732)283
InitiationofACE-IorARBContinueRAASBlockade.Accept<25%fallinGFR.Ensureitisnotprogressive.Goal130/80ReviewMedicationsDietaryK+RestrictionDiureticAddsecondagentDiureticNon-dihydroperidineCCBBetaBlocker
GoalProteinuriaIndependentRiskMarkerThereforeNeedsIndependentTherapeuticGoalIrrespectiveofBPControlProteinuriaDoseResponsetoRAASBlockadeMayNotParallellThatofBP
GoalProteinuria<300mg/24hoursorRatioof<0.3RAASBlockadeBPControl±ProteinRestriction
CaseExample56yearoldBachelorFarmerTypeIIDMMx2yearsRetinopathyProteinuriaLivingaloneHighsaltintakeReferredformanagementofrisingserumcreatinine
CaseExampleMedicationsBasalBolusInsulinAmlodipine10mgdaily24hoururinarysodium160mmol/L
01/200509/200601/200702/2009Creat87120140247eGFR78564723PCRBP160/90165/95165/93170/95CaseExample
RelationshipbetweenBPControlandRateofDeclineinGFRBakrisetalAJKD,2000.
Interventions:Tightsaltrestriction(100mmol/5g)NoaddedsaltNosaltincookingMinimisepre-preparedfoodRamipril5mg40/3mmHgBPdropCaseexample
01/200509/200601/200702/200904/200907/200902/201006/2010Creat87120140247268270260298eGFR7856472321212219PCR2.80.60.70.1BP160/90165/95165/93170/95160/75135/70130/70122/72CaseExampleNephrologyReferral
CaseExample
‘Givingupthesaltmadeanawfuldifference’‘Saltisapoison!’‘Bytheway,DrHorgantellsmemyeyesarewaybetter’Caseexample
SummaryInproteinuricCKDACE-inhibition+5gsaltrestrictionDiuretic(thiazideorloop~eGFR)Non-dihydropyridineCCBOthersGoal<130/80mmHgatleastARBinTypeIIDMorifACEi→cough
SummaryInnon-proteinuricCKD5gsaltrestrictionACE-inotmandatoryDiuretic(thiazideorloop~eGFR)Non-dihydropyridineCCBOthersGoal<130/80mmHg?BewareARVD
Questions?